
Healthy Parenting
Local approaches to a worldwide problem
Year: 2018-2020
Duration: 3 projects: Kids Healthy Plate Singapore, (6 month), Healthy ETE-ing Rotterdam (3 months) and Healthy Parenting Rotterdam (6 months).
Client: Design for Impact initiated the projects ‘Healthy ETE-ing Rotterdam’ and ‘Healthy Parenting Rotterdam’. Both were partly funded by DesignScapes. Among our partners were: the city council of Rotterdam, SWK Group, Erasmus MC department of Public Health, CJG Rijnmond, Alsare.
In Singapore our project ‘Kids Healthy Plate’ was initiated by KK Women’s and Children’s Hospital.
My role: Initiator, design researcher, strategic designer.
Impact: In both countries we designed context specific new perspectives of helping tackle childhood obesity.
In Singapore we co-created a family challenge supported by a Healthy plate for kids of different ages and placemats to communicate the challenge goals. The tools help parents educate their kids on healthy portions and supports them in making it fun and easy to stick to the portions suggested. Prototypes of the Healthy plate tools were produced to create further buy-in within KK Hospital to continue this project.
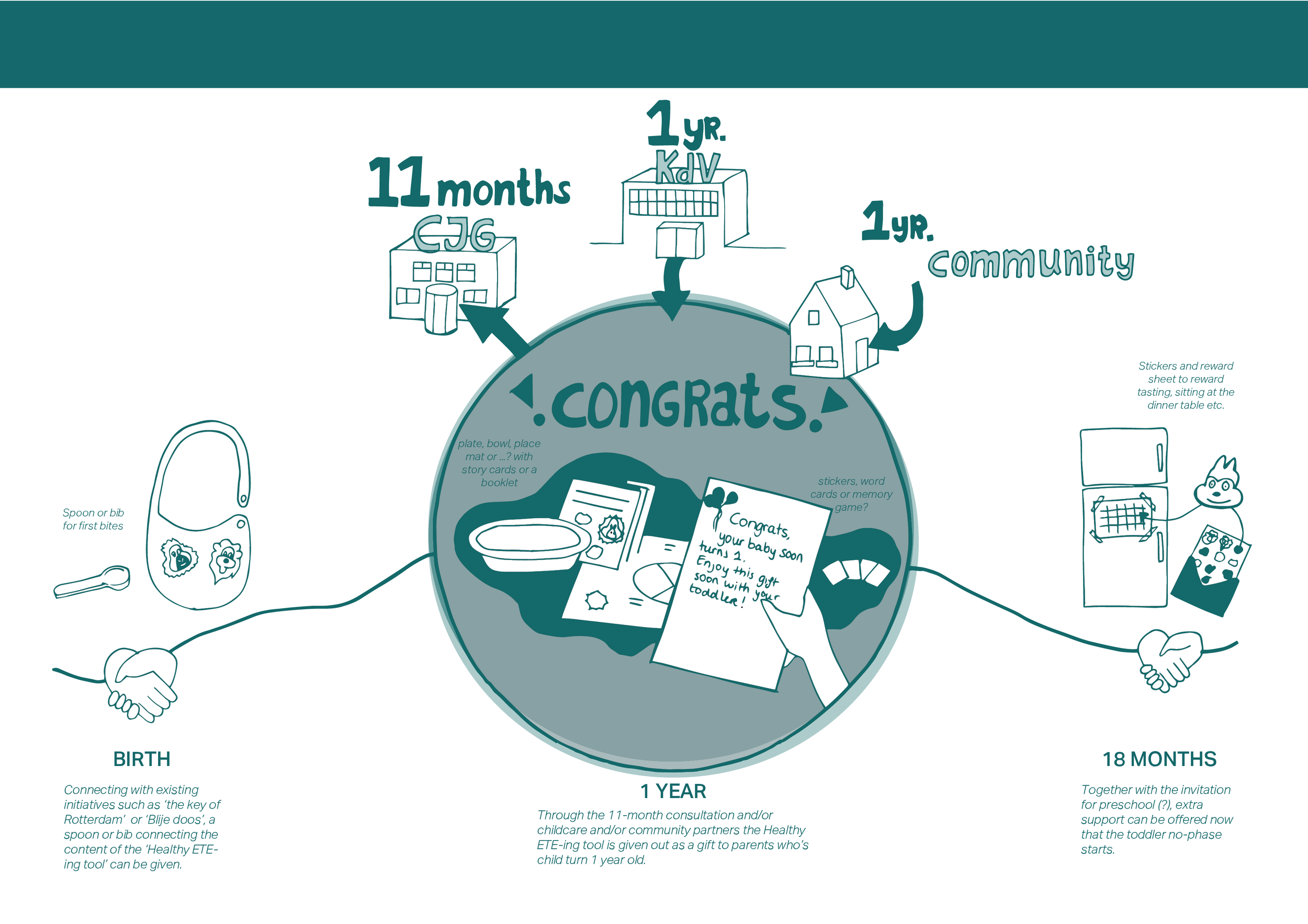
In Rotterdam we designed (in 2020) the SUPER-eater gift set which focusses on parents of young children (1 year old) and helps them create a SUPER eater out of their child. The gift set shifts focus from ‘healthy eating’ to ‘easy eating’, something all parents strive for. The gift set translates and embodies parenting practices in practical and visual tools so that they can be put to practice. A short impact study showed possible positive behaviour change in parents who received the gift set. Furthermore, the gift set is able to reach – and embody healthy messages- to target groups whom previously could not be reached. Back stage this project connected diverse organisations around this topic and opened up perspectives for helping solve this problem together (cross-organisation & multi-stakeholder). At the moment we are searching for ways to finance the way forward; how do we make implementation possible starting from a shared value model?

The SUPER eater gift set: By addressing the needs of parents (need to feel valued for parenting, to be approached in a positive manner and to experience easy dinners with young kids), parents are motivated to follow up on the advocated SUPER eater practices. The SUPER eater practices are all simply worded and each can be found on a practical tool that makes adherence to the practice easier. The gift set shifts focus from ‘healthy eating’ to ‘easy eating’, something all parents strive for. The gift set translates and embodies parenting practices in practical and visual tools so that they can be put to practice. This way, the set enables parents to use authoritative parenting practices, which are associated with lower rates of obesity, and makes meal time easier and more fun for both parents and children. Although the set doesn’t prescribe what is healthy or good, the set triggers reflection on healthy eating in a low-key way.
Problem: Child obesity is a growing problem. In Rotterdam 1 out of 4 (!) children are overweight, in Singapore this is 1 out of 8. Furthermore, according to the Dutch National Food Consumption Survey (by RIVM) only 19% of the Dutch 2-year olds and 16% of adults eat enough vegetables. In Singapore, only half of schoolchildren eat the recommended two servings each of fruit and vegetables a day. Both excessive amounts and lack of variety in food intake are important determinants of obesity. Without intervention there is a high chance that obese children turn into obese adults.
Challenge: Despite the many interventions in Rotterdam around healthy lifestyle there are little to no interventions which aim for universal prevention from an early age focussing on the home setting. Many interventions are offered at paid day care or at schools and aim for educating parents though the knowledge of their children. Most interventions focus on cognition and materials for parents are highly textual. However, from the young age of 1-year old, children join in the family dinners and eating and parenting practices are established. Between the age of 1 and 4 years old many parents lack support and offered support feels stigmatising and is often experienced as paternalistic. Parents from lower socio-economic background are not being reached by the current interventions and programs as they are far from their lived-reality.
In Singapore too the challenge is to reach parents from a lower-economic background, for whom English is not their mother tongue. Health-literacy and time among this group is low and families often dine out where portions do not match with the daily recommended intake. Furthermore, abundance is considered wealthy.
Direction: Among the many factors that play a part in growing rates of obesity we focused on influencing unhealthful choices through parenting practices.
In Rotterdam an analysis of existing programs and interventions revealed little to no emphasis on supporting parenting practices despite proven effectiveness in interventions targeted at parents from obese children. To quote the Netherlands Youth Institute: “There is an opportunity developing an intervention which promotes the authoritative child rearing style”. Authoritative parenting practices are associated with lower rates of obesity.
We saw an opportunity for: a visual, tangible & practical universal prevention tool to be used at home, which nudges young parents & toddlers to eat balanced meals and promotes authoritative upbringing practices in parents, helps parents make more healthful choices for their children.
In Singapore a lot less programs and interventions existed. The Health Promotion Board and MOH (ministry of health) Obesity Clinical Guidelines advise behavioural modifications that influence weight status e.g. healthy eating habits should be emphasised for weight management in children and adolescents.
Process Rotterdam: First a feasibility study was conducted followed by a prototyping phase. Expert generative interviews and benchmarking were used to analyse the current state. A stakeholder session helped frame a perspective for a future state and directions were co-created into a concept design. This concept design was prototyped (low-fidelity) during the prototyping phase and used as input for user co-creation. 21 mothers and 3 behaviour and public health experts co-created their versions of a tangible practical too. The design was iterated based on all co-creation learnings and 35 high fidelity prototypes were created. A short-term impact study was done in collaboration with the Erasmus Medical School. Results show possible positive behaviour change.



Value model Rotterdam: Impact of the set will take place in the future and multiple stakeholders will benefit if the set helps to change behaviour sustainably. However, costs for the set are now. Who is going to pay for the set and who is benefitting? How can we measure long term impact and effect? These are questions we want to explore in the future; how can we come to a financing model together, between different organisations with different short-term stakes? We have explored some of these stakes during our feasibility study and we want to continue to build a shared value model together.






Process Singapore: In Singapore we co-created together with paediatricians, dieticians and primary care nurses. We then designed a first concept which we showed to families to gather their input. The concept was then iterated together with the team. Prototypes were produced and additional feedback was gathered.